

SB535: The Law That Liberates Longevity
Montana could become the blueprint for preventative medicine



Infinita is collecting interest for providers of therapies and clinicians to join its efforts to build a longevity haven in Montana. Apply to deploy under SB 535 (RFP)
On May 12, 2025, the Montana state legislature passed a law. Laws are notoriously difficult to read, and rarely raise excitement - this one you should pay attention to.
There are 30+ state right-to-try (R2T) laws, including a federal one from 2018. Montana is special, if you care about longevity and medical freedom.
#1 Longevity Compatibility
It was prior legislation, Montana’s SB 422 in October 2023, that is the more radical change. It broadens patient eligibility from the terminally-ill to… everyone.
EVERYONE.
This is an enormous breakthrough for longevity medicine, which is preventative in nature, as opposed to the prevalent healthcare system of symptom palliation.
#2 A Clear Pathway
The new bill is on the face of it more technical in nature. More focused on the implementation and market infrastructure side of things. That does not make it less transformative.
SB 535 is not only “deregulation”. It maintains safeguards and even adds in new ones (such as a stricter informed consent process). More importantly, it streamlines a complex and uncertain regulatory path for providers to enter the market and patient access under R2T.
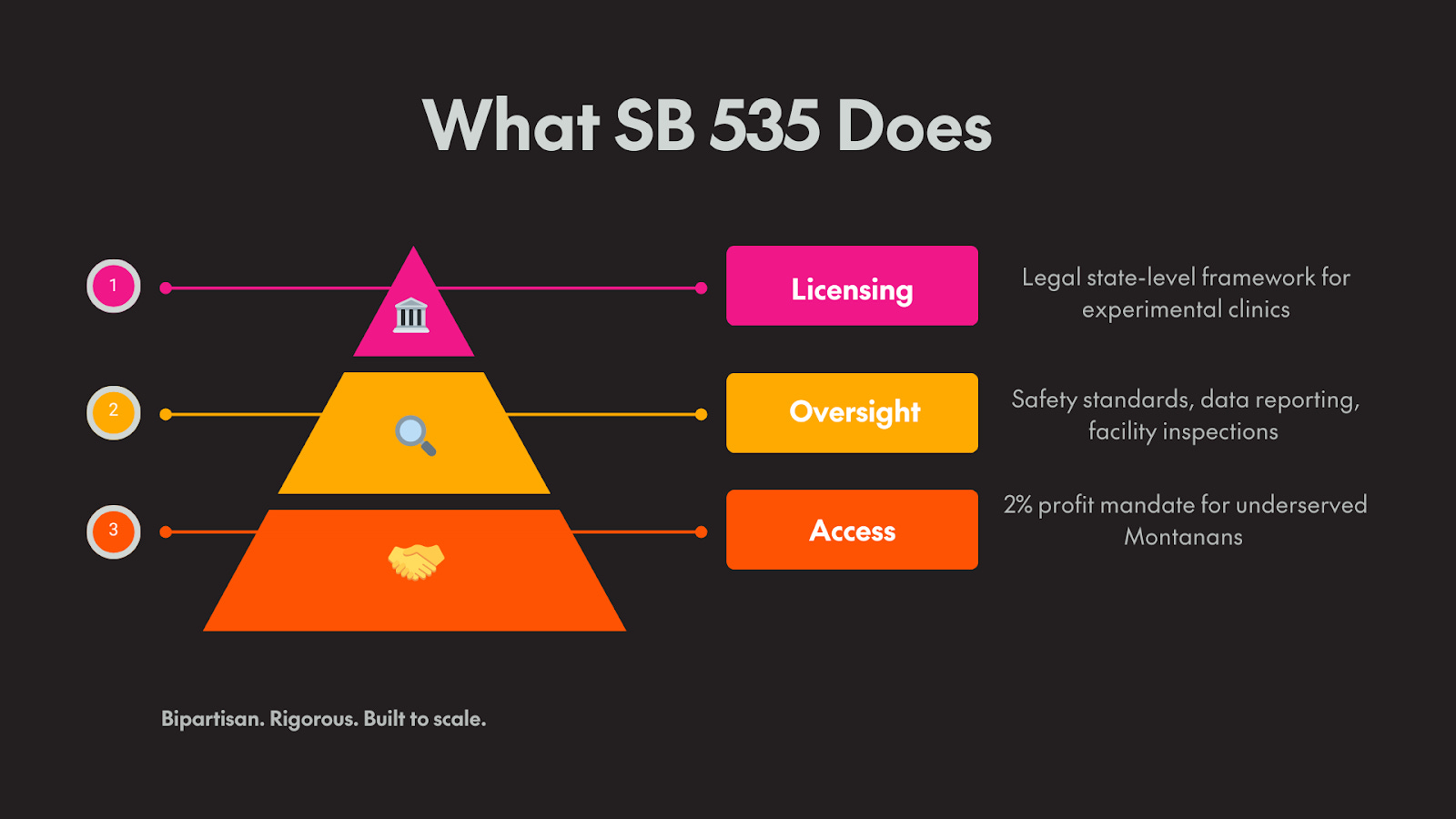
The key tenets of SB 535 are the following:
Streamlining: the law creates a new category of “Experimental Treatment Centers” (ETC), and exempts it from insurance and payments regulations. These areas have nothing to do with medical safety, but in practice form a bottleneck & commercial constraints for new providers. This makes things focused on actual safety, under clear oversight by Montana’s department for health and human services (DPHHS).
Market Expansion: the law adds more clarity for provider protections, reducing risk for US-based providers in active clinical investigation. Beyond that, it clarifies the pathway for international providers with proven therapies to enter the US market - this is already implicitly possible under federal right-to-try, but just wasn’t made explicit before.
Direct-to-Patient: by adding payment flexibility, defining provider contracts, and in addition to Montana’s past efforts to allow direct contracting between healthcare providers and patients, removes middlemen and third-party payments. It allows pay-out-of-pocket models, which allow faster market access for providers - with flexible insurance arrangements on top, but not a precondition for treatment.
This makes it a model legislation that other states could follow.
A Safe Harbor within the US Healthcare Regulatory Maze
In 2012, a group of analysts led by Jack Scannell coined a bitter inversion of Moore’s Law. Where computing became exponentially cheaper and faster, biomedicine became slower, riskier, and more expensive. They called it Eroom’s Law.
Insulin reached patients just six months after its discovery in the 1920s. Penicillin scaled globally in under three years. Today, a new therapy takes more than a decade and costs over $500 million to reach the market.
This is certainly a key factor in pushing the internal rate of return on pharma R&D below the cost of capital.

Pharma’s R&D is structurally broken. The returns have been falling for 30 years - dropping below the cost of capital. SB535 is one of the few legal mechanisms designed to reverse that trend.
Scientific progress didn't stall. Neither did demand for medical services.
It’s the institutions that slowed down adoption. And it’s not just the FDA, it’s multiple layers of third-parties that stand between patients and medical innovation.
The FDA in many ways added professionalism and rigor into the process. The past is not a “golden age” in all ways. Patient safety was often neglected in research.
Yet it certainly overshot in the other direction and disallowed risk-taking and decentralized adoption, an often messy process but the hallmark of innovation.
The cost of compliance makes important new discoveries or existing technology commercially infeasible. Startups now build their timelines around regulation, not patients. Innovation is done pre-market - and stays there. For most founders, this is accepted reality. You raise more money. You hire regulatory consultants. You wait, you research, you sell to big pharma.
A group of longevity advocates and a champion state senator looked for a different path.
Montana: Not a Coincidence
Montana has a tradition of embracing self-reliance, a pro-business governor, and neighbors like Idaho and Wyoming that treat deregulation as economic strategy.
It’s also becoming a "next Colorado" for coastal expats - especially founders and tech talent - who started moving during the pandemic.
Previously, Montana had already deregulated the onerous “certificate of need” requirements for clinics and opened up direct provider to patient contracting, and pro-crypto laws.
Montana has an appetite for growth and progress.
Montana Senator Ken Bogner spearheaded the legislative efforts to attract industries of the future, with the first SB 422 law that invited the longevity industry to the state.
Unfortunately there have not been results since October 2023 when SB 422 passed, but Bogner was not discouraged. Instead he invited more longevity industry representatives to come and learn what else would be needed to make market entry commercially attractive.
Bogner’s persistence and willingness to iterate led to SB 535.
Montana is now ready to be a longevity haven.

What About the Risks?
Critics say that allowing people to access therapies after just one Phase I trial is reckless. They cite the failure rate: over 90% of clinical drug candidates never make it to market.
But this statistic overlooks a few important things:
Not all drugs are rejected for the right reasons; they may work in specific patient groups, or in different combinations. They have been rejected within a rigid framework with external selection criteria (that are often pre-scientific) with high costs of iteration.
The single indication requirement precludes a lot of promising longevity treatments, or combinatorial therapies from even making it to trials; the pathway to market is the so called “1-to-n” model, one drug or treatment to 1.000s of people - however the alternative model of “n-to-1” to systematically research multiple different approaches to combat a disease, or aging itself, is much harder to do within the current constraints.
There are drugs and treatments approved abroad, with abundant safety and efficacy data - but they’re not recognized by the FDA for various reasons, from bureaucratic inertia, bias against certain therapeutic areas, and potentially also regulatory capture from industry interests
The failures are not just because the drugs are unsafe or ineffective. Many fail because the system is too slow, too expensive, or too inflexible to accommodate iteration.
The ones suffering most from this inertia are patients that are terminally-ill, and for whom waiting for approval may mean certain death - even a 10% chance may be worth taking.
A less morally recognized group is the emerging longevity industry, that aims to treat diseases before they occur. This approach just falls outside the cracks of the regulatory system.
While the image of healthy biohackers aiming to live longer may not be politically the most appealing, the industry as a whole is simply aiming for something big: what if we can develop treatments that make you live 20-30 years longer, instead of 2-3 years? That is a scientific and technological possibility. A lot of new innovation looks unappealing and risky in the beginning, but now we’re all grateful that the internet, credit cards, space technology, combustion engines, airplanes etc. exist. Longevity is a truly disruptive paradigm, looking for a regulatory and legal safe harbor to innovate in safely - Montana is set to become this Longevity Safe Harbor.

The cost of waiting is rarely accounted for. But it is always paid.
Technology and Regulatory Change
The passage of SB 535 was a hallmark case of regulatory innovation.
Bradley Tusk who developed Uber's regulatory and media strategy, Eli Dourado’s work with Boom Supersonic or the case of Zipline, the drone delivery company that saves mothers’ lives in Rwanda to prove the safety of its technology.
New technology often runs up against regulations that lock in old technology. Regulations are notoriously hard to change - but now with artificial intelligence (AI) it has become a lot easier. It allows synthesizing large and complex amounts of data so that different stakeholders can align and make more informed decisions, guided by the democratic process.
Montana proves to be a true frontier state. It may enter history as the state that liberated longevity, in an exemplary process where technology and democracy work together.
The framework exists. Now it needs builders.
If you're ready to test and deploy, the door is open:
→ Apply to deploy under SB 535 (RFP)
→ Read the bill (full text)
→ Read the A4LI announcement
→ Apply to deploy under BIO/ACC
